|
Case Report
Granulocyte-colony-stimulating-factor (G-CSF) producing hepatocellular carcinoma with rapid progression: A case report
1 Center of Gastroenterology and Oncology, IMS Ota Chuo General Hospital, Ota, Japan
2 Department of General Surgery, Flash Hospital, Fujioka, Japan
3 Department of Pathology, Gunma Prefectural Cancer Center, Ota, Japan
4 Department of General Surgery, Cleveland Clinic Foundation, Cleveland, OH, USA
5 Department of General Surgery, Itabashi Chuo Medical Center, Tokyo, Japan
6 Department of Diagnostic Pathology, Dokkyo University Hospital, Japan
Address correspondence to:
Yuhei Nakano
Center of Gastroenterology and Oncology, IMS Ota Chuo General Hospital, 371-8513 875-1 Higashi-imaizumi-machi, Ota-shi, Gunma,
Japan
Message to Corresponding Author
Article ID: 100016G01YN2021
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Nakano Y, Ohwada S, Kashima Y, Matsuyama H, Kawate S, Iijima M, Moro A, Sasaki K, Yoshimura Y, Nakajima R, Takada-Owada A. Granulocyte-colony-stimulating- factor (G-CSF) producing hepatocellular carcinoma with rapid progression: A case report. Edorium J Gastroenterol 2021;8:100016G01YN2021.ABSTRACT
Introduction: This is a case of an 80-year-old man presented a large hepatocellular carcinoma (HCC) and portal vein tumor thrombus (PVTT) extending to the bifurcation of the portal vein (PV). He had leukocytosis and elevated serum G-CSF. Although the patient underwent en bloc PV tumor thrombectomy followed by right hepatectomy, he died of hepatic hilar lymph nodes and multiple lung metastases two months after surgery. Pathological findings showed poorly differentiated HCC and positive G-CSF immunostaining. Clinicians are in need to note the management for HCC with concurrent G-CSF producing and PVTT. Granulocyte-colony-stimulating-factor (G-CSF) producing hepatocellular carcinoma (HCC) has been reported as a rare and poor prognosis tumor. Further, PVTT is also a poor prognostic factor in HCC. We report a case of G-CSF producing HCC with PVTT that progressed rapidly to die soon after surgery.
Case Report: An 80-year-old man presented anorexia and fatigue. Abdominal computed tomography (CT) scan showed a large liver tumor in the right lobe and PVTT extending to the bifurcation of the PV. He had leukocytosis and elevated serum G-CSF. The patient underwent en bloc PV tumor thrombectomy followed by right hepatectomy, but his leukocytosis did not normalize. He died of hepatic hilar lymph nodes and multiple lung metastases two months after surgery regardless of complete tumor removal. Pathological findings showed poorly differentiated HCC and positive G-CSF immunostaining.
Conclusion: Clinicians are in need to note the management for HCC with concurrent G-CSF producing and PVTT.
Keywords: Granulocyte-colony-stimulating-factor, Hepatocellular carcinoma, Leukocytosis, Portal vein tumor thrombus, Surgery
INTRODUCTION
The granulocyte colony-stimulating factor (G-CSF)-producing tumor is referred to as one of the paraneoplastic syndromes and has been detected in lung cancer, bladder cancer, sarcoma, cervical cancer of the uterus, and gallbladder cancer [1]. In these organs, G-CSF-producing tumors proliferate and have a poor prognosis. It is reported by the studies that G-CSF progress the tumor cell growth in vitro and has been tightly linked to tumor generation and progression in many tumor types [2],[3],[4]. Granulocyte colony-stimulating factor producing hepatocellular carcinoma (HCC) is rare and known for its poor prognosis. In addition, HCC is prone to invade the portal venous system, and approximately 10–60% of HCC patients have portal vein tumor thrombus (PVTT) at the time of diagnosis [5]. The prognosis of HCC with PVTT patients is much poor; their overall survival is only 2–4 months with supportive care [6].
Hepatocellular carcinoma with PVTT was known to be a contraindication of surgery. However, recent reports suggested that complete tumor removal might benefit oncological prognosis in selected patients [7]. The optimal indication or absolute contraindication of PV tumor thrombectomy in HCC is still unclear, although many researchers attempted to elucidate. This report presents a rare case of a G-CSF producing HCC coexisted with PVTT extending to the bifurcation of PV. Herein, we discuss the management of G-CSF producing HCC and HCC with PVTT. We also explored the previous literature of surgical G-CSF producing HCC cases, including our case.
CASE REPORT
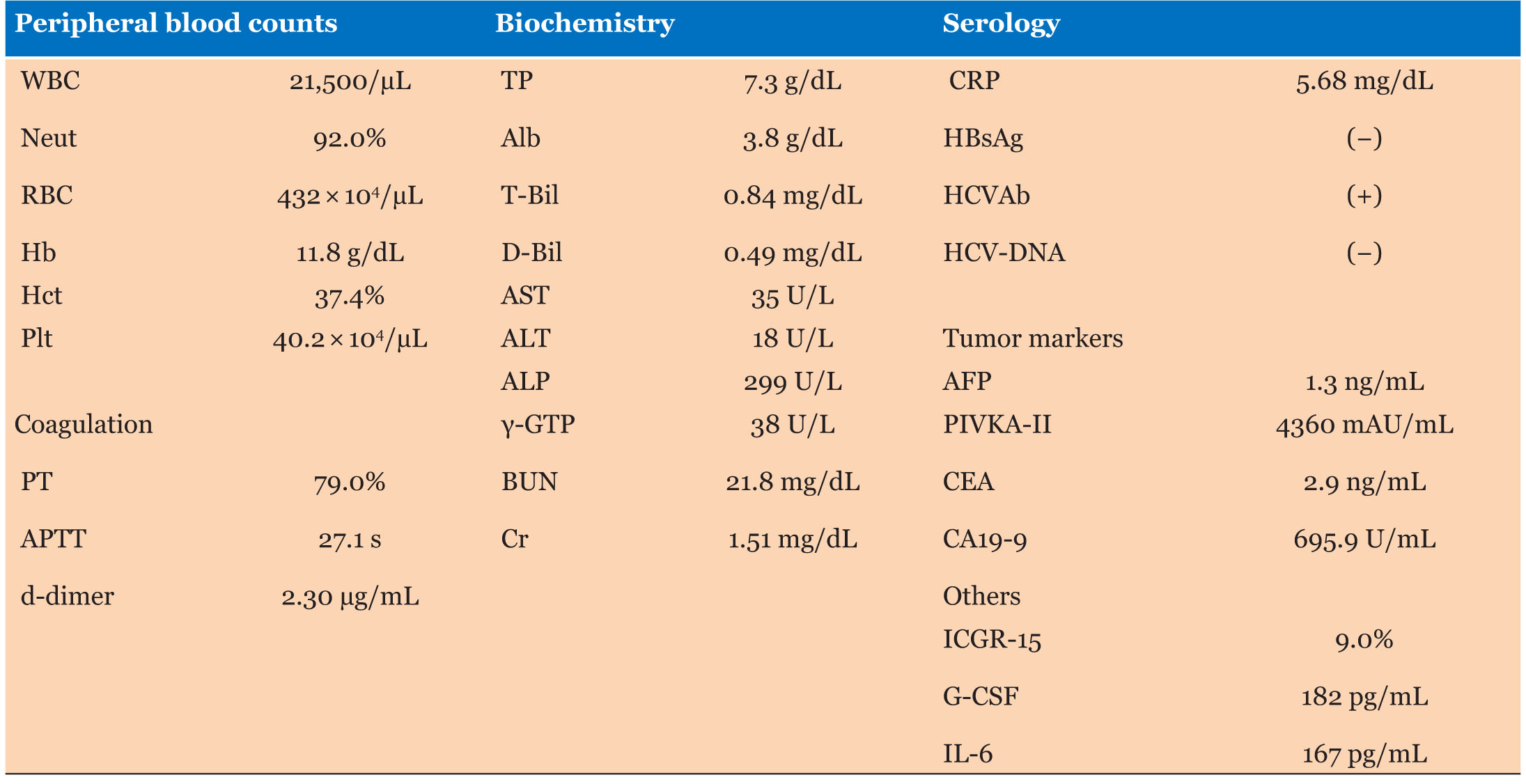
An 80-year-old man visited our hospital because of anorexia and fatigue. He had a history of acute hepatitis C virus (HCV) infection from blood transfusions during surgery for a traumatic injury 50 years ago, although the HCV was spontaneously resolved. He was treated with interferon and hepatitis virus was completely cured. He also had prostate cancer, which has been well controlled with Goserelin acetate (Zoladex) for 5 years. The laboratory data upon admission were as follows: White blood cell count (WBC) 28,300/μL, C-reactive protein (CRP) 5.7 mg/dL, total-bilirubin (T-bil) 0.84 mg/dL, aspartate aminotransferase (AST) 35 U/L, alanine aminotransferase (ALT) 18 U/L, lactate dehydrogenase (LDH) 249 U/L, alkaline phosphatase (ALP) 299 U/L, gamma-glutamyltransferase (GGT) 38 U/L, α-fetoprotein (AFP) 1.3 ng/mL, protein induced by the absence of vitamin K (PIVKA)-II 4360 mAU/mL. Hepatitis B surface antigen (HBsAg) was negative. He was positive for HCV antibody (4.17 S/CO) with a negative HCV-RNA polymerase chain reaction (PCR) (Table 1).
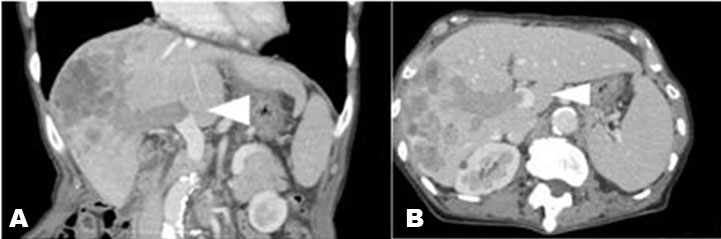
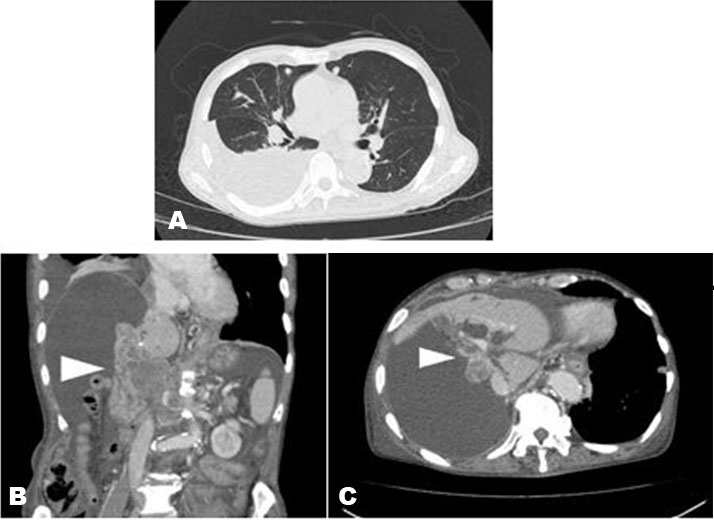
An upper and lower gastrointestinal endoscopy showed no abnormality. Computed tomography (CT) and abdominal ultrasound showed a large hypodense tumor with ring enhancement, central necrosis, and daughter nodules in the right lobe. Computed tomography also documented the portal vein tumor thrombus extending to the bifurcation (Figure 1A and Figure 1B). Neither the lung nor lymphoid metastases were seen. His mild fever, leukocytosis, and CRP were attributed to central necrosis of the large HCC and distal obstructive cholangitis. Although initially treated with antibiotics, WBC did not decrease. There was a possibility that the PVTT would spread further, extending to the main portal vein, and obstruct the whole vein lumen, resulting in liver failure or life-threatening variceal bleeding. We assessed the functional hepatic reserve as follows, Indocyanine green (ICG) 9.0%, Indocyanine green plasma clearance rate (KICG) 0.141, Albumin bilirubin (ALBI) score −0.27 (2a), Child-pugh score 5 (A), and Model for End-Stage Liver Disease (MELD)-Na score 8 (estimated 3-months mortality 1.9%). The functional liver reserve was evaluated to tolerate right liver resection and portal vein tumor thrombectomy. We took an informed consent about the surgical risk and the prospective of his cancer without surgery. We discussed in our cancer board and decided to precede liver resection and portal vein tumor thrombectomy with postoperative administration of a multi-kinase inhibitor.
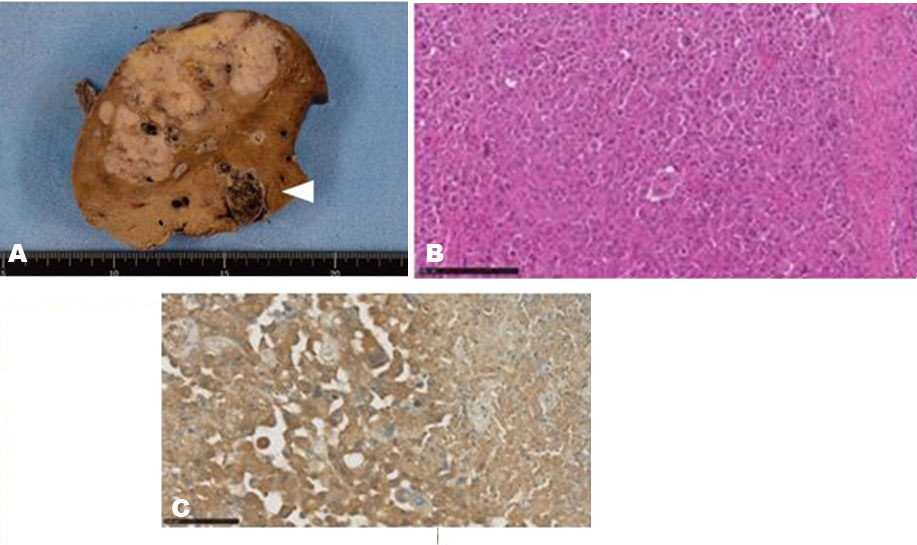
We performed en bloc portal tumor thrombectomy following with right hepatectomy. Partial hepatic resection of S2 was added for a single 0.5 × 0.5 cm tumor detected by intraoperative ultrasound. The resected tumor size of 12.8 × 5.9 cm occupied the right liver lobe, and the cut surface showed a yellowish-white, multi-nodular fusion type without capsule, and central necrosis. Portal tumor thrombosis and multiple daughter nodules were also seen (Figure 2A). Histological examination revealed that the tumor was mostly composed of histologically poorly/moderately differentiated HCC (Figure 2B). The patient was diagnosed as HCC with grade VP3 PVTT, VV1, B0 stage IV. The surgical margin was negative. The liver background had a slight fatty change.
After surgery, his WBC count decreased to 12,000/μL but did not normalize. He was discharged from the hospital 18 days after surgery. One month after surgery, he was readmitted for loss of appetite, fatigue, and mild jaundice. White blood cell count was elevated up to 51,600/μL, which was suspicious for G-CSF production. The serum G-CSF was 182 pg/mL (normal range: <39.0 pg/mL), and Interleukin (IL)-6 was 167 pg/mL (normal range: <4.0 pg/mL). The blood test showed: T-bil 8.5 mg/dL, AST 448 U/L, ALT 227 U/L, LDH 314 U/L, ALP 2,833 U/L, and GGT 234 U/L. Immunohistochemically, the tumor cells were positive for G-CSF staining (Figure 2C). Computed tomography revealed multiple lung metastases (Figure 3A) and hilar lymph node metastasis, resulting in obstructive jaundice (Figure 3B and Figure 3C). His general condition deteriorated rapidly due to progressive liver failure and acute renal failure. He died two months after surgery. So we couldn’t use multi-kinase inhibitor.
DISCUSSION
We experienced a G-CSF producing large HCC with PVTT extending to the main PV bifurcation. This case met the diagnostic criteria for G-CSF-producing tumors [8],[9]; marked increased WBC count, elevated G-CSF activity, and verification of G-CSF production in the tumor. The tumor recurred invasively in a short period after an en bloc portal vein tumor thrombectomy and right hepatectomy regardless of complete tumor removal (R0 resection). The patient died two months after surgery with multiple metastases. This case provides an instructive lesson in the management of G-CSF producing HCC with PVTT, which are two poor prognostic factors.
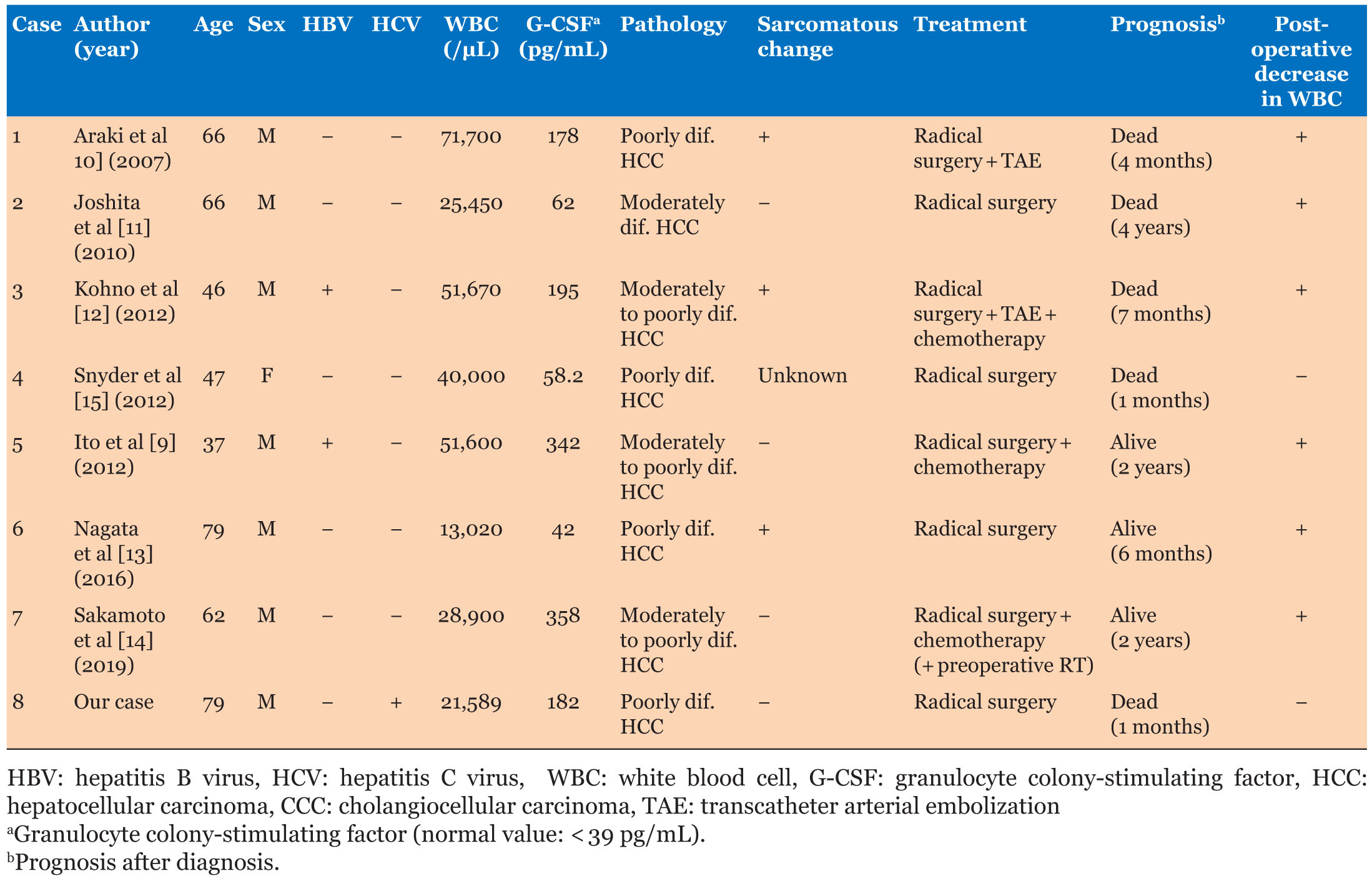
We reviewed international literature of eight surgical resection cases of G-CSF producing HCC (Table 2) [9],[10],[11],[12],[13],[14],[15]. The previous seven cases were diagnosed before surgery. The current case was diagnosed postoperatively with GCS-F production HCC due to the findings of the high WBC count (more than 50,000/μL), elevated serum G-CSF (182 pg/mL) and Interleukin (IL)-6 (167 pg/mL), confirmed by an immunohistochemically positive test for G-CSF. Seven out of the eight cases were male, and two patients had positive hepatitis B virus. Most HCCs progressed rapidly with a median tumor size of 10 cm. Two cases had invaded the stomach and large intestine, and our case had PVTT. Most cases were initially treated with antibiotics, although the WBC did not decrease. As such, when patients are negative for hepatitis virus, have a tumor larger than 10 cm, low-grade fever, WBC counts that are not responding to antibiotics, and are men, it is essential to note G-CSF-producing HCC as a differential diagnosis.
Whether radical surgery is an effective strategy or not for G-CSF producing HCC is still controversial. Six out of eight patients underwent major hepatectomy, and two underwent combined gastrectomy or colon resection. Three patients received sorafenib after relapse. There were recurrences in seven cases. Five of the seven recurrent cases recurred in the liver, lungs, bones, and hilar lymph nodes within two months after surgery. One case recurred in the lung within eight months after surgery, and another case recurred in the bone within three years after surgery. The prognosis of the case of Joshita et al. [11] was the longest with four years, and the cases of Ito et al. [9] and Sakamoto et al. [14] survived for two years. Postoperative WBC counts normalized in six cases, but Synder et al. [15] and the current case did not normalize. In the case of Snyder et al., the patient died at one month postoperatively due to radical lymphatic and pulmonary metastases. Our patient died two months postoperatively due to hepatic hilar lymph node metastasis resulting in obstructive jaundice and portal vein compression. Our case also had small lung metastases.
This case had an additional dismal prognostic factor of PVTT. There is no internationally accepted consensus or guideline for diagnosis and treatment of HCC with PVTT. Western and Asian countries have taken a completely opposite view to treat HCC with PVTT. In Japan and China, HCC with PVTT is not a contradiction in the surgical approach. Patients with PVTT up to the first branch are considered to undergo en bloc hepatectomy and tumor thrombectomy of curative intent if the remaining liver has an acceptable functional reserve, the lesion is resectable, and there is no extrahepatic metastasis [16]. In our case, the PVTT extended to the PV bifurcation, and the liver function reserve was sufficient for right hepatectomy and tumor thrombectomy [8]. In contrast, according to the Barcelona Clinic for Liver Cancer (BCLC) staging system, HCC with PVTT is recognized as an advanced stage disease (BCLC stage C). Surgical resection is not a recommended treatment, and the tyrosine kinase inhibitors sorafenib and regorafenib have been proposed as the only treatment options. Both the American Association for the Study of Liver Disease (AASLD) and the European Association for the Study of Liver Disease (EASL) have accepted the treatment algorithm for BCLC. The extent of PVTT is closely related to the prognosis of HCC. In patients with PVTT extending to or beyond the bifurcation, the 1-, 3-, and 5-year overall survival rates were 50%, 12.5%, and 12.5%, respectively [17]. These survival outcomes were satisfactory when compared with those of patients with PVTT who were untreated or sorafenib alone, or transarterial chemoembolization (TACE) combined sorafenib. Even using sorafenib, we can hardly extend the prognosis over one year. The median overall survival of untreated and receiving sorafenib is 4.1 months and 5.6 months, respectively [18].
The Eastern Hepatobiliary Surgery Hospital (EHBH)-PVTT score system is reported to be able to predict the prognosis in HCC patients with PVTT after R0 liver resection [19]. Median overall survival of an EHBH-PVTT score ≤3 patients showed better survival of 19.0 months, compared to 8.9 months for an EHBH-PVTT score >3. EHBH-PVTT score of our patient was 3 and died two months after R0 liver resection. The management of G-CSF producing HCC with PVTT can be challenging. It is evident that the patient’s prognoses and outcomes with PVTT and G-CSF producing HCC vary from those of patients without them. Selected patients may benefit from a more aggressive treatment approach. On the other hand, not all patients may uniformly benefit from aggressive treatment. Therefore, when facing patients with HCC with PVTT and/or G-CSF producing HCC, clinicians must balance the potential benefits and risks of different treatments individually. A multidisciplinary tumor board is required to determine the most appropriate management of patients with PVTT and/or G-CSF production. Future studies should focus on combinations of different established treatment modalities for PVTT and/or G-CSF producing HCC.
CONCLUSION
We report a case of G-CSF producing HCC with PVTT that progressed rapidly to die soon after R0 portal tumor thrombectomy followed with hepatectomy. Management of HCC with PVTT and/or G-CSF producing is a clinical dilemma with challenges. If we would see a patient with those two poor prognostic factors, surgical treatment can’t be recommended, in our opinion.
REFERENCE
1.
Asano S, Urabe A, Okabe T, Sato N, Kondo Y. Demonstration of granulopoietic factor(s) in the plasma of nude mice transplanted with a human lung cancer and in the tumor tissue. Blood 1977;49(5):845–52.
[Pubmed]

2.
Nakata H, Uemura Y, Kobayashi M, Harada R, Taguchi H. Cyclooxygenase-2 inhibitor NS-398 suppresses cell growth and constitutive production of granulocyte-colony stimulating factor and granulocyte macrophage-colony stimulating factor in lung cancer cells. Cancer Sci 2003;94(2):173–80. [CrossRef]
[Pubmed]
3.
Mattei S, Colombo MP, Melani C, Silvani A, Parmiani G, Herlyn M. Expression of cytokine/growth factors and their receptors in human melanoma and melanocytes. Int J Cancer 1994;56(6):853–7. [CrossRef]
[Pubmed]
4.
Baba M, Hasegawa H, Nakayabu M, et al. Establishment and characteristics of a gastric cancer cell line (HuGC-OOHIRA) producing high levels of G-CSF, GM-CSF, and IL-6: The presence of autocrine growth control by G-CSF. Am J Hematol 1995;49(3):207–15. [CrossRef]
[Pubmed]
5.
Zhang ZM, Lai ECH, Zhang C, et al. The strategies for treating primary hepatocellular carcinoma with portal vein tumor thrombus. Int J Surg 2015;20:8–16. [CrossRef]
[Pubmed]
6.
Zhang X, Wang K, Wang M, et al. Transarterial chemoembolization (TACE) combined with sorafenib versus TACE for hepatocellular carcinoma with portal vein tumor thrombus: A systematic review and meta-analysis. Oncotarget 2017;8(17):29416–27. [CrossRef]
[Pubmed]
7.
Cheng S, Chen M, Cai J, et al. Chinese expert consensus on multidisciplinary diagnosis and treatment of hepatocellular carcinoma with portal vein tumor thrombus (2018 edition). Liver Cancer 2020;9(1):28–40. [CrossRef]
[Pubmed]
8.
Ohwada S, Kawate S, Hamada K, et al. Perioperative real-time monitoring of indocyanine green clearance by pulse spectrophotometry predicts remnant liver functional reserve in resection of hepatocellular carcinoma. Br J Surg 2006;93(3):339–46. [CrossRef]
[Pubmed]
9.
Ito T, Okubo K, Shiomi M, et al. A case of successful treatment of granulocyte colony-stimulating factor producing hepatocellular carcinoma accompanying type B hepatitis with tegafur-uracil. [Article in Japanese]. Nihon Shokakibyo Gakkai Zasshi 2012;109(12):2088–96.
[Pubmed]
10.
Araki K, Harimoto N, Yamanaka T, et al. Efficiency of regional functional liver volume assessment using Gd-EOB-DTPA-enhanced magnetic resonance imaging for hepatocellular carcinoma with portal vein tumor thrombus. Surg Today 2020;50(11):1496–506. [CrossRef]
[Pubmed]
11.
Joshita S, Nakazawa K, Koike S, et al. A case of granulocyte-colony stimulating factor-producing hepatocellular carcinoma confirmed by immunohistochemistry. J Korean Med Sci 2010;25(3):476–80. [CrossRef]
[Pubmed]
12.
Kohno M, Shirabe K, Mano Y, et al. Granulocyte colony-stimulating-factor-producing hepatocellular carcinoma with extensive sarcomatous changes: Report of a case. Surg Today 2013;43(4):439–45. [CrossRef]
[Pubmed]
13.
Nagata H, Komatsu S, Takaki W, et al. Granulocyte colony-stimulating factor-producing hepatocellular carcinoma with abrupt changes. World J Clin Oncol 2016;7(5):380–6. [CrossRef]
[Pubmed]
14.
Sakamoto Y, Kamiyama T, Yokoo H, et al. Hepatocellular carcinoma producing granulocyte colony-stimulating factor: Diagnosis and treatment. Int Cancer Conf J 2018;8(1):12–6. [CrossRef]
[Pubmed]
15.
Snyder RA, Liu E, Merchant NB. Granulocyte colony stimulating factor secreting hepatocellular carcinoma. Am Surg 2012;78(7):821–2. [CrossRef]
[Pubmed]
16.
Cheng S, Chen M, Cai J; National Research Cooperative Group for Diagnosis and Treatment of Hepatocellular Carcinoma with Tumor Thrombus. Chinese expert consensus on multidisciplinary diagnosis and treatment of hepatocellular carcinoma with portal vein tumor thrombus: 2016 edition. Oncotarget 2017;8(5):8867–76.
[Pubmed]
17.
Chan SL, Chong CCN, Chan AWH, Poon DMC, Chok KSH. Management of hepatocellular carcinoma with portal vein tumor thrombosis: Review and update at 2016. World J Gastroenterol 2016;22(32):7289–300. [CrossRef]
[Pubmed]
18.
Cerrito L, Annicchiarico BE, Iezzi R, Gasbarrini A, Pompili M, Ponziani FR. Treatment of hepatocellular carcinoma in patients with portal vein tumor thrombosis: Beyond the known frontiers. World J Gastroenterol 2019;25(31):4360–82. [CrossRef]
[Pubmed]
19.
Zhang XP, Gao YZ, Chen ZH, et al. An eastern hepatobiliary surgery hospital/portal vein tumor thrombus scoring system as an aid to decision making on hepatectomy for hepatocellular carcinoma patients with portal vein tumor thrombus: A multicenter study. Hepatology 2019;69(5):2076–90. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Acknowledgement
We appreciate Kenzo Okauchi, Department of Diagnostic Radiology, who supported us to diagnose as G-CSF producing HCC.
Author ContributionsYuhei Nakano - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Susumu Ohwada - Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Yasushige Kashima - Analysis of data, Drafting the work, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Hideki Matsuyama - Analysis of data, Drafting the work, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Susumu Kawate - Analysis of data, Drafting the work, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Misa Iijima - Analysis of data, Drafting the work, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Amika Moro - Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Kazunari Sasaki - Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Yukino Yoshimura - Analysis of data, Drafting the work, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Ryuichiro Nakajima - Analysis of data, Drafting the work, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Atsuko Takada-Owada - Analysis of data, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guarantor of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2021 Yuhei Nakano et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.