|
Case Report
Glomus tumor in duodenum: A pericytic tumor at unusual location
1 Department of Pathology, United Christian Hospital, Hong Kong
Address correspondence to:
Shui-ying Cheng
Department of Pathology, United Christian Hospital,
Hong Kong
Message to Corresponding Author
Article ID: 100018G01GL2022
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Lo C-h, Cheng S-y. Glomus tumor in duodenum: A pericytic tumor at unusual location. Edorium J Gastroenterol 2022;9:100018G01GL2022.ABSTRACT
Introduction: Glomus tumor is a neoplasm composed of perivascular modified smooth muscle cells of the normal glomus body. Rarely, it has been reported in the gastrointestinal tract. The vast majority are benign, with malignant behavior reported in two cases of gastric glomus tumors.
Case Report: We present here a case of glomus tumor originated from duodenum, which was found incidentally in imaging. Histopathological examination and immunohistochemical studies confirmed the presence of glomus tumor. This article illustrates a case of glomus tumor at duodenum, with discussion on its differential diagnosis and management approach.
Conclusion: The pathologist needs to be aware of the histology features of glomus tumor. The definitive diagnosis relies on histological assessment. Based on the typical morphology and the help of immunohistochemical study, glomus tumor can usually be confidently diagnosed.
Keywords: Duodenum, Glomus tumor, Pericytic tumor
INTRODUCTION
Glomus tumor is a benign neoplasm composed of perivascular modified smooth muscle cells of the normal glomus body. Most of them occur as a soft tissue neoplasm in the distal extremities, such as the subungual region, hand, wrist, and foot [1]. Rarely, it has been reported in the gastrointestinal tract, in which the vast majority arise within the stomach [2]. Glomus tumor arising from the intestine is exceedingly rare, with only a few case reports available in English literature [3],[4],[5],[6],[7],[8],[9],[10]. Herein we describe a case of glomus tumor arising in the duodenum.
CASE REPORT
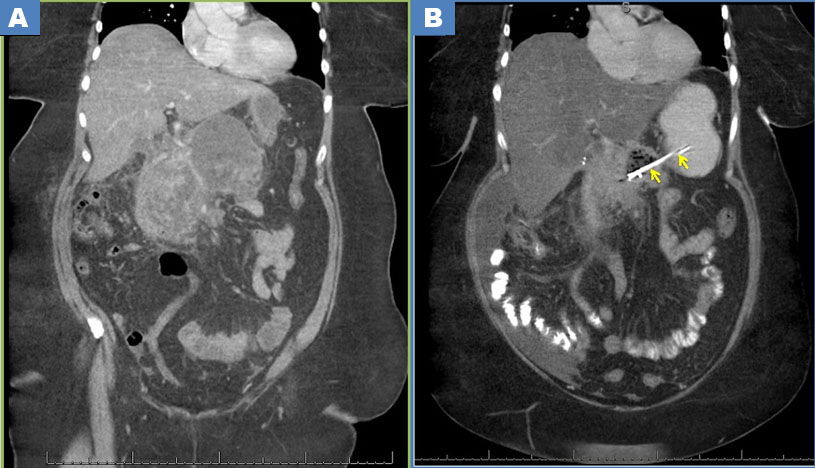
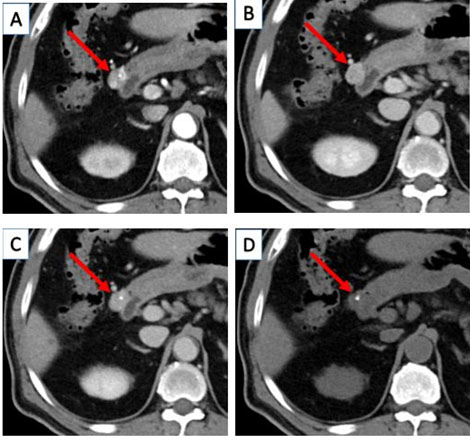
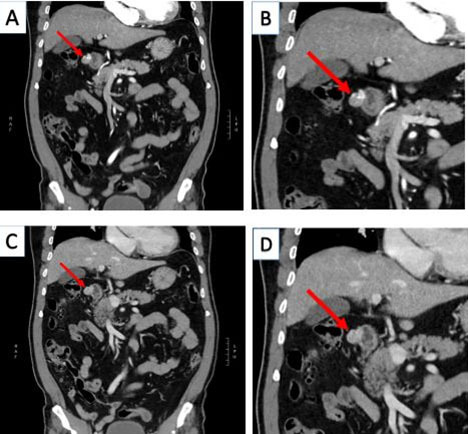
A 70-year-old Chinese man, with history of colonic diverticulosis, presented with episodes of fresh per-rectal bleeding and hemoglobin drop from 10.6 to 7.8 g/dL. Proctoscopy showed minimal internal hemorrhoids. Colonoscopy showed multiple diverticula over entire colon without any mucosal lesion. A diagnosis of diverticular bleeding was made. However, computed tomography (CT) scan of the abdomen and pelvis showed an incidental finding of a 1.8 cm roundish lesion at the anterior wall of duodenal bulb, in additional to diffuse diverticulosis of colon. The lesion showed early intense arterial enhancement which persisted into portal venous and later phases, and a tiny focus of internal calcification (Figure 1 and Figure 2).
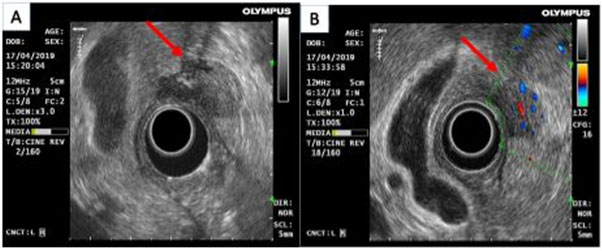
Subsequent endoscopic ultrasound was performed to further delineate the lesion, which showed a 2 cm hypoechoic lesion at the first part of duodenum. It appeared to be arising from muscularis propria layer of duodenal wall with increasing Doppler signal and internal calcification (Figure 3).
The clinical and radiological impression at that moment was a duodenal gastrointestinal stromal tumor, with other differential diagnoses including neuroendocrine tumor, hemangioma and glomus tumor. The lesion was then circumferentially excised via laparoscopic approach, and the defect was transversely closed and reinforced with tongue of tension-free omentum. The tumor was sent for histopathological examination.
Gross examination
Received was a piece of duodenal wall tissue measuring 2 × 2 × 1 cm in size, with the overlying mucosa measuring 1 × 1 cm in area. A tan color submucosal nodule was identified on sectioning, measuring 1.7 × 1.5 × 1 cm.
Microscopic examination
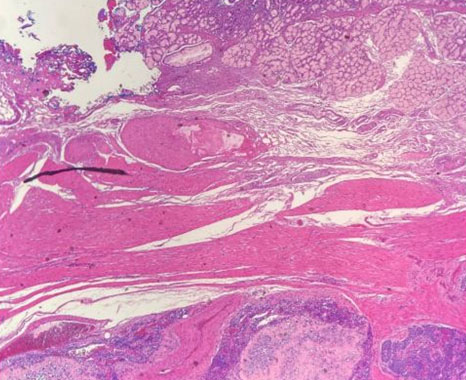
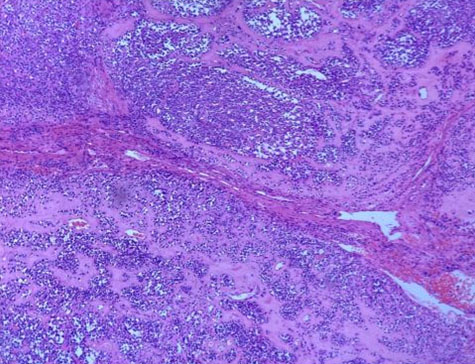
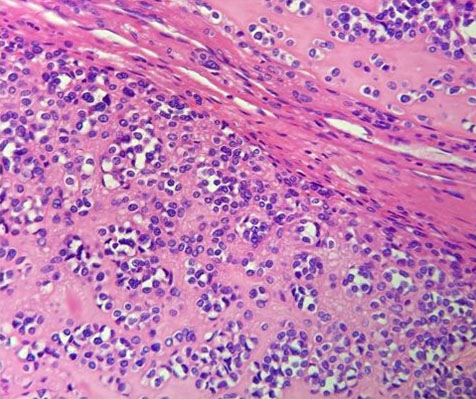
Sections showed duodenal tissue with a well-defined, non-encapsulated lesion arising from the muscular propria. It was composed of tumor cells arranged in nests, cords, or isolation, and separated by delicate vascular channels. The tumor cells were roundish with fair amount of eosinophilic cytoplasm, mild hyperchromatic nuclei, and inconspicuous nucleoli. Mitosis was not identified. A focus of calcification was present. The overlying duodenal mucosa was unremarkable. The resection margin is clear by 3 mm microscopically (Figure 4, Figure 5, Figure 6).
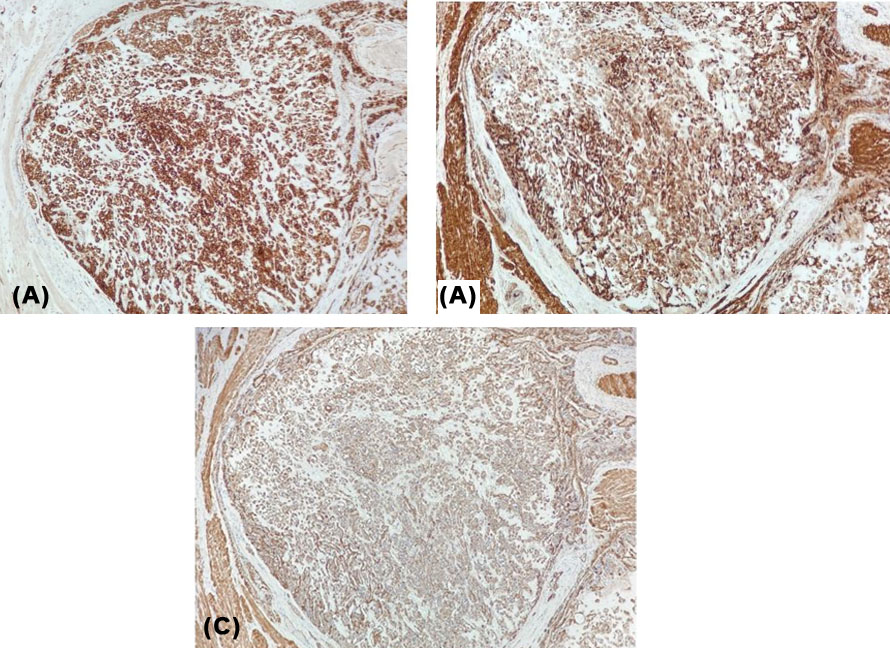
Immunohistochemical study showed that the tumor cells were diffusely positive for smooth muscle actin, caldesmon, and synaptophysin. MNF116, Cam 5.2, AE1AE3, DOG1, S100, and c-kit are negative. The Ki-67 labeling index was about 1% (Figure 7).
The overall features were consistent with glomus tumor arising from duodenum.
Progress
The surgery was uneventful and the patient remained well with no signs of recurrence after 18 months of surgery.
DISCUSSION
Glomus tumor in the gastrointestinal tract is uncommon, in which the vast majority arise within the stomach. Glomus tumor arising from the intestine is exceedingly rare, making accurate preoperative diagnosis difficult. The differential diagnoses of a hypervascular tumor in contrast-enhanced computed tomography (CT) scan include gastrointestinal stromal tumor, neuroendocrine tumor, hemangioma and glomus tumor.
In microscopic examination, the diagnosis is relatively straight forward. Typical glomus tumor involves the muscularis propria, and is composed of uniform, small round cells with a discrete round nucleus and pale to eosinophilic cytoplasm. The cells are arranged in sheets and nests with a rich vascular network. The stroma is typically myxoid or hyalinized. Mitotic activity is usually low. Focal nuclear atypia and vascular invasion can be observed, and vascular invasion does not affect prognosis.
Immunohistochemically, glomus tumor is almost always diffusely and strongly positive for smooth muscle actin. Caldesmon is also positive in more than half of the cases. Focal synaptophysin expression has also been reported [2],[11],[12]. However, in our case, diffuse and strong positive for synaptophysin is observed. This may be a potential diagnostic pitfall in the differential diagnosis with neuroendocrine tumor. The importance of the use of a panel of immunostains cannot be overemphasized.
The vast majority of gastrointestinal glomus tumor is benign. However, malignant behavior has been reported in two cases of gastric glomus tumors that metastasized to the liver. Both were larger than 5 cm, and one showed mild atypia, spindle cell foci (1 and 2). No malignant behavior has been reported in duodenal glomus tumor.
Nevertheless, the criteria for malignancy in gastrointestinal tract are undefined due to insufficient data. The criteria for malignancy for peripheral soft tissue glomus tumor are deep location and size >2 cm, or atypical mitotic figures, or moderate to high nuclear grade and ≥5 mitoses/10 mm2 [1].
CONCLUSION
Herein we describe a Chinese case of glomus tumor arising in the duodenum. An accurate pre-operative diagnosis is difficult. Contrast-enhanced computed tomography (CT) scan may show strong arterial enhancement and prolonged enhancement in portal venous phase with a hemangioma-like enhancement pattern. The definitive diagnosis relies on histological assessment. Based on the typical morphology and the help of immunostains, glomus tumor can usually be confidently diagnosed. Glomus tumor should be included in the differential diagnosis list among the submucosal tumors.
REFERENCE
1.
Folpe AL, Fanburg-Smith JC, Miettinen M, Weiss SW. Atypical and malignant glomus tumors: Analysis of 52 cases, with a proposal for the reclassification of glomus tumors. Am J Surg Pathol 2001;25(1):1–12. [CrossRef]
[Pubmed]

2.
Miettinen M, Paal E, Lasota J, Sobin LH. Gastrointestinal glomus tumors: A clinicopathologic, immunohistochemical, and molecular genetic study of 32 cases. Am J Surg Pathol 2002;26(3):301–11. [CrossRef]
[Pubmed]
3.
Sasaki S, Takami Y, Wada Y, et al. Glomus tumor of the duodenum: A rare case report. Surg Case Rep 2020;6(1):305. [CrossRef]
[Pubmed]
4.
Yoon J, Kim K, Lee S. Imaging findings of glomus tumor at duodenum: A case description. Quant Imaging Med Surg 2020;10(5):1133–7. [CrossRef]
[Pubmed]
5.
Jundi M, Lack EE, Brun EA, Esquivel J, Kumar D. Glomus tumor of the duodenum: A case report. Int J Surg Pathol 2004;12(4):411–4. [CrossRef]
[Pubmed]
6.
Sadidoust A, Anbardar MH, Lankarani KB. Endoscopic mucosal resection of a glomus tumour of the duodenum. Prz Gastroenterol 2020;15(2):173–4. [CrossRef]
[Pubmed]
7.
Hur BY, Kim SH, Choi JY, et al. Gastroduodenal glomus tumors: Differentiation from other subepithelial lesions based on dynamic contrast-enhanced CT findings. AJR Am J Roentgenol 2011;197(6):1351–9. [CrossRef]
[Pubmed]
8.
Shelton JH, Lamont JP, Zieske A, Mallat DB. Glomus tumor of the ampulla. Gastrointest Endosc 2007;66(2):395–6.
[Pubmed]
9.
Knackstedt C, Wasmuth H, Donner A, Trautwein C, Winograd R. Diagnosis of an unusual tumor in the duodenum. Endoscopy 2007;39 Suppl 1:E94. [CrossRef]
[Pubmed]
10.
Jundi M, Lack EE, Brun EA, Esquivel J, Kumar D. Glomus tumor of the duodenum: A case report. Int J Surg Pathol 2004;12(4):411–4. [CrossRef]
[Pubmed]
11.
Wang JC, Jin XF, Weng SX, Xu C, Gan MF. Gastric glomus tumors expressing synaptophysin: Clinicopathologic and immunohistochemical analyses. [Article in Chinese]. Zhonghua Bing Li Xue Za Zhi 2017;46(11):756–9. [CrossRef]
[Pubmed]
12.
Meguro S, Kusama Y, Matsushima S, et al. Nasal glomus tumor: A rare nasal tumor with diffuse and strongly positive synaptophysin expression. Pathol Int 2019;69(11):672–4. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Author Contributions
Chun-hai Lo - Analysis of data, Drafting the work, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Shui-ying Cheng - Conception of the work, Design of the work, Acquisition of data, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guarantor of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2022 Chun-hai Lo et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.