|
Case Report
Imaging findings in thrichobezoars: A case report
1 Faculty of Medicine and Pharmacies of Rabat, Medical Imaging Services for Maternity and Children, University Hospital Center, Rabat, Morocco
Address correspondence to:
Arthur Semedo Insumbo
Faculty of Medicine and Pharmacies of Rabat, Medical Imaging Services for Maternity and Children, University Hospital Center, Rabat,
Morocco
Message to Corresponding Author
Article ID: 100014G01AI2021
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Insumbo AS, Chalh O, Allali N, El Haddad S, Latifa C. Imaging findings in thrichobezoars: A case report. Edorium J Gastroenterol 2021;8:100014G01AI2021.ABSTRACT
A rare case of bezoar extending from the stomach to the small intestine or beyond has been described as Rapunzel syndrome. Bezoars are concretions in the gastrointestinal tract with enormous potential to increase in size by continuous accumulation of undigested material or non-absorbable food and fibers. Most bezoars in children are trichobezoars from dolls and swallowed hair from the head or brushes. The typical clinical presentations of trichobezoars are abdominal pain and nausea, but can also present as an asymptomatic abdominal mass, able to progress giving rise to complication such as abdominal obstruction and perforation. Trichobezoar with Rapunzel syndrome is an uncommon diagnosis in children with very few reported cases. It is often found in emotionally disturbed or mentally retarded youngsters. We present the youngest case of Rapunzel syndrome in Morocco, a 5-year-old boy without any antecedent who presented with abdominal pain, vomiting, and abdominal mass.
Keywords: Abdominal mass and computed axial tomography (CAT), Pediatric, Rapunzel syndrome, Trichobezoar
INTRODUCTION
Bezoars are accumulations of undigested material (human or vegetable fibers) in the gastrointestinal tract. It is known that the word bezoar comes from the Arabic word bedzehr or Persian word padzahr, meaning “protecting against poisons.” In history, bezoars from animal guts were used as precious stones and antidotes to poisons. Until today traditional Chinese medicine still uses it for preventing and treatment of cerebral vascular spasm [1].
In 1779, the first reference to a bezoar in a human was described during an autopsy of a patient who died from gastric perforation and peritonitis [2],[3].
Bezoars have been classified according to their primary constituents: hair (trichobezoars), medications (pharmacobezoars), vegetable or fruit fiber (phytobezoars), milk curd (lactobezoars), persimmon fiber (diospyrobezoars), and miscellaneous materials (plastic gloves, paper tissue, etc.) [2]. In humans, the most common type of bezoar is the trichobezoar, which is mostly made of hair. The most common bezoars in children are trichobezoars [3].
Bezoar cases occur more in the first three decades of life, mostly in patients with an underlying psychiatric disorder [4].
This entity is known as Rapunzel syndrome which is a rare form of trichobezoar in the stomach with some extension into the small intestine [1]. The syndrome is named after a fairy tale written in 1812 by the Brothers Grimm about the young maiden Rapunzel, who lowered her long hair to the ground in her prison tower to permit a prince to climb up and rescue her [2]. The syndrome was first described by Vaughan et al. in 1968, and it is an uncommon diagnosis in children, with fewer than 40 cases reported in the literature [5],[6].
We report the case of a young boy with Rapunzel syndrome in Morocco that presented with abdominal pain and an epigastric mass.
CASE REPORT
A 5-year-old boy with the weight of 18 kg was presented in our service with a month of slow-on abdominal pain and three days of postprandial emesis. He always complained of pain after every meal and then felt relief after vomiting. Also he appeared to be in some discomfort but was able to communicate by sign language.
His parents commented on chronically decreased appetite and early satiety. There was no history of diarrhea, recent illnesses, fever, acid reflux, or increased flatulence. There were no changes in his bowel habits. On examination, there was no alopecia. When directly asked, the patient admitted that he liked to eat hair. In the physical exam performed on the abdomen revealed a hard mass of approximately 15 cm × 10 cm, fixing in the central region of the epigastrium and lateralizing to the right, extending into the right upper quadrant (Figure 1 and Figure 2B). He also presented exaggerated bowel sounds. The rest of the physical examination was normal.
Simple abdominal radiography of the abdomen showed multiple air fluid levels (Figure 1). There were no major changes in the laboratory tests performed, only some urine concentrates were revealed. Complete blood count, complete metabolic panel, as well as pancreatic enzymes were normal, and nothing else.
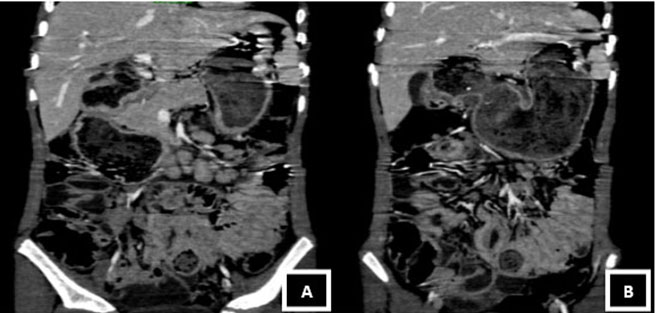
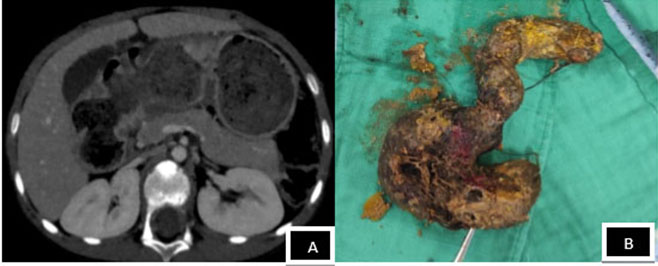
For a confirmation of the diagnosis and considering the large size of the abdominal mass and showed multiple air fluid levels on X-ray, the abdominal computed tomography (CT) with contrast were performed. The CT confirmed large presence of a heterogeneous hypodense mass with mottled material inside it taking the shape of the stomach and exerting compression on its wall. This mass continues and extends even in the small intestine (duodenal and jejune region) measuring approximately 20 × 6 cm, believed to be bezoar (Figure 2 and Figure 3). In the days after diagnosis a gastrotomy was performed and the mass was removed in one piece. The 17 cm × 8 cm × 6 cm mass was found to be a trichobezoar with a tapering tail extending into the small bowel, and was a perfect cast of the stomach, pylorus, and duodenal bulb taking the typical shape of these structures (Figure 2). Rests of the abdomen organs were normal. After seven days the patient was discharged home, having recovered without complications. Psychiatric follow-up was arranged, where he showed improvement in behavior, which is key to avoid recurrence of his condition or better to prevent recurrence.

DISCUSSION
Bezoars, also known as Rapunzel syndrome, are concretions of foreign material in the gastrointestinal tract, affecting mainly the stomach and small intestine as in our patient. Bezoars are composed generally of hair or hair-like fibers are called trichobezoars. Most patients with trichobezoars suffer from psychiatric disorders including trichotillomania (pulling out of their own hair) and trichophagia (eating of hair). Much evidence estimates that only 1% of patients with trichophagia develops a trichobezoar [7],[8]. It is described that trichobezoars form when hair strands, escaping peristaltic propulsion because of their slippery surface, and are retained in the folds that constitute internal walls of the gastric mucosa. As more hair accumulates, with the process of peristalsis these materials will be rolled up and adopting the shape of a ball. As this ball gets too large to leave the stomach, gastric atony may result. The ball of hair becomes even more matted together and takes the shape of the stomach space, usually as a single solid mass [9],[10].
We conclude that the frequent location of these casts in the stomach is due to the blockage caused mainly by the pyloric valve associated with the stomach agitation action that further facilitates the tangling of new hair into the already formed cast. We can also notice the shiny aspect of its external surface from the mucus that covers it. Usually over time the decomposition and fermentation of fats give the bezoar, and the patient’s breathe a putrid smell [11]. Also the denaturalization of hair protein by the action of stomach acid gives the bezoar its black color [12],[13].
Clinical presentation it depends not only on the duration but mainly on the size of trichobezoar. As bezoars enlarge with time, a variety of symptoms also develop, such as abdominal discomfort and pain, early satiety, postprandial fullness, nausea, and vomiting. Other clinical presentations can be observed namely iron-deficiency anemia. In our case, the bezoar was large; however, the little boy reported only minor abdominal pain and early satiety. Also large bezoars can cause serious complications, such as gastric outlet obstruction, obstructive jaundice, gastrointestinal bleeding, protein-losing enteropathy, acute pancreatitis, small-intestine obstruction as reported in our patient, perforation, peritonitis, and intussusceptions. Therefore, it is important to emphasize that recognition and timely treatment of the bezoar are of major importance [14].
Diagnostic imaging studies are usually performed in patients not only with possible complications, but also in patients with nonspecific upper gastrointestinal symptoms. Through imaging studies trichobezoars are detectable as mass lesions within the stomach, as was also the case in our patient (Figure 2 and Figure 3). In Rapunzel syndrome, CT is important for estimating the extension of the trichobezoar into the small intestine, meanly duodenum and jejunum.
Upper gastrointestinal endoscopy is usually performed to confirm the diagnosis and to reveal the constituents of the bezoar. In some types of bezoars, such as phytobezoars and lactobezoars, endoscopy can be effective in diagnosis and therapeutic intervention option to eliminate the bezoar [15]. In our case, endoscopy was not performed because a clear diagnosis of the size and extension of the bezoar was achieved by using CT imaging. It is known that trichobezoars cannot be removed though an endoscopic procedure due to their size and consistency [16].
Treatment is essentially surgical. The extraction of the bezoar through laparotomy is done with exploration of rest of the small intestine for the purpose of certifying the presence of detached bezoars.
In our patient, surgical treatment was gastrotomy and the trichobezoar mass was removed in one piece. At the time of surgery there was the trichobezoar extension into the duodenum with a larger detached part of bezoar distally within the intestine (Figure 3B). The extension of the trichobezoar in the duodenum diagnosed by CT was provided. Laparoscopic removal of a trichobezoar could be a surgical option; however, it may be hard to achieve when trichobezoars are large [17].
CONCLUSION
Trichobezoar is a rare entity almost under-diagnosed. Clinically it presents abdominal pain and a non-tender abdominal mass even in young children, and is always accompanied by the history of pica. Many of these patients may have psychiatric problems. In young boys with psychiatric history who present with abdominal pain, vomiting or abdominal mass, bezoars/Rapunzel syndrome should be considered in the differential diagnosis. For a confirmation of the diagnosis the X-ray and CT abdominal with contrast is needed to perform the diagnostic. Bezoars like Rapunzel syndrome, the treatment consists essentially in surgical removal. In cases of small trichobezoar the treatment may be done by endoscopic extraction of the fragment, gastric lavage, enzymatic therapy, or combinations of these approaches.
REFERENCE
1.
Wang C, Zhao X, Mao S, Wang Y, Cui X, Pu Y. Management of SAH with traditional Chinese medicine in China. Neurol Res 2006;28(4):436–444. [CrossRef]
[Pubmed]

2.
Naik S, Gupta V, Naik S, Rangole A, Chaudhary AK, Jain P, Sharma AK. Rapunzel syndrome reviewed and redefined. Dig Surg 2007;24(3):157–61. [CrossRef]
[Pubmed]
3.
Sanders MK. Bezoars: From mystical charms to medical and nutritional management. Practical Gastroenterology. 2004. [Available at: https://med.virginia.edu/ginutrition/wp-content/uploads/sites/199/2015/11/Sanders-Jan-04.pdf]
4.
Grimm Brothers: Rapunzel. Translated by Godwin-Jones R. Richmond, Virginia Commonwealth University Department of Foreign Languages, 1994–1999.
5.
Vaughan ED Jr, Sawyers JL, Scott HW Jr. The Rapunzel syndrome. An unusual complication of intestinal bezoar. Surgery 1968;63(2):339–43.
[Pubmed]
6.
Emre AU, Tascilar O, Karadeniz G, Irkorucu O, Karakaya K, Comert M. Rapunzel syndrome of a cotton bezoar in a multimorbid patient. Clinics 2008;63(2):284–8.
7.
Phillips MR, Zaheer S, Drugas GT. Gastric trichobezoar: Case report and literature review. Mayo Clin Proc 1998;73(7):653–6. [CrossRef]
[Pubmed]
8.
Irving PM, Kadirkamanathan SS, Priston AV, Blanshard C. Education and imaging. Gastrointestinal: Rapunzel syndrome. J Gastroenterol Hepatol 2007;22(12):2361. [CrossRef]
[Pubmed]
9.
Pace AP, Fearne C. Trichobezoar in a 13 year old male: A case report and review of literature. Malta Med J 2003;15:39–40
10.
Deslypere JP, Praet M, Verdonk G. An unusual case of the trichobezoar: The Rapunzel syndrome. Am J Gastroenterol 1982;77(7):467–70.
[Pubmed]
11.
Sidhu BS, Singh G, Khanna S. Trichobezoar. J Indian Med Assoc 1993;91(4):100–1.
[Pubmed]
12.
Sharma V, Sahi RP, Misra NC. Gastrointestinal bezoars. J Indian Med Assoc 1991;89(12):338–9.
[Pubmed]
13.
O’Sullivan MJ, McGreal G, Walsh JG, Redmond HP. Trichobezoar. J R Soc Med 2001;94(2):68–70.
[Pubmed]
14.
Sharma P, Kumar S, Kumar B, Jadon RS. Rapunzel syndrome: A rare cause of vomiting and pain abdomen. JK Science 2012;14(3):146–8.
15.
Gonuguntla V, Joshi DD. Rapunzel syndrome: A comprehensive review of an unusual case of trichobezoar. Clin Med Res 2009;7(3):99–102. [CrossRef]
[Pubmed]
16.
Kaushik NK, Sharma YP, Negi A, Jaswal A. Image-gastric trichobezoar. Indian J Radiol Imaging 1999;9(3):137–9.
17.
Jatal SN, Jamadar NP, Jadhav B, Siddiqui S, Ingle SB. Extremely unusual case of gastrointestinal trichobezoar. World J Clin Cases 2015;3(5):466–9.
[Pubmed]
SUPPORTING INFORMATION
Author Contributions
Arthur Semedo Insumbo - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Olaya Chalh - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Nazik Allali - Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Siham El Haddad - Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Chat Latifa - Analysis of data, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guarantor of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2021 Arthur Semedo Insumbo et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.